CIRS: A New Paradigm for Chronic Disease | Part 3
Understanding the Biotoxin Pathway & Lab Tests for Diagnosis

Aaron Hartman MD
January 8, 2019

Subscribe
Never miss out on new content from Dr. Hartman.
After my initial evaluation appointment with Steve at our Functional Medicine Practice In Richmond, Virginia, I wasn’t quite sure how to proceed. His main diagnosis was Hashimoto’s Hypothyroidism, but he had already gone gluten free, seen an endocrinologist and felt no better. All his symptoms started after a tick bite and rash that was correctly diagnosed as Lyme Disease and then treated appropriately with antibiotics. But he hadn’t gotten any better and had already seen two ‘Lyme literate’ physicians without any improvements. I had recently started to study Mold-Related Biotoxin Illness (aka CIRS) and wondered if this might be the underlying cause for all his maladies. So, I pulled out my lab sheet and drew 15 vials of blood for analysis. When I got the results back my head started to spin. Now what? How do I interpret c4A levels and all the bizarre and relatively unknown labs?
This article will be technical. I am going to review the full Biotoxin Pathway and the associated labs. While this section is geared towards practitioners, a well-educated patient who has read the previous information and links should be able to grasp the basic concepts and become a partner in their health care. Let’s begin!
New!
Interactive Infographic
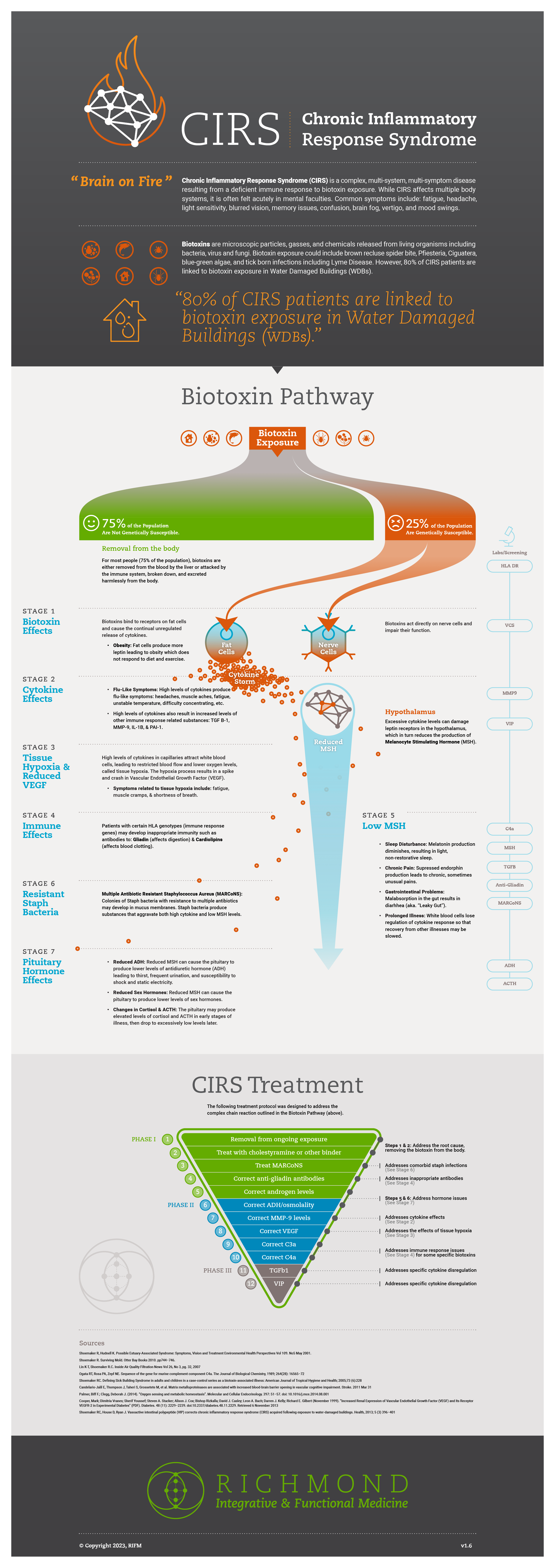
After several years working with an older diagram, we have created a new one that better outlines the complex chain reaction in body systems set off by biotoxin exposure. For visual learners, you can click hotspots in the diagram to link back to explore other resources from this series.
Part Three
Understanding the Biotoxin Pathway & the Labs Behind Its Evaluation

First, an individual must be exposed to a biotoxin from a source. For 75% of the population who are not genetically susceptible (aka HLA DR/DQ susceptible), these toxins are labelled by the immune system and either broken down by the immune system or tagged for removal and harmlessly removed by the liver through secretion into the bile and elimination from the body. For the rest of us, it is difficult to remove these toxins, they can slowly build up in our system and then begin to affect our immune and nervous system.
Theses biotoxins act directly on nerve cells and impair their function. This process is detectable early by a test call the Visual Contrast Sensitivity Test. At the same time, the toxins will bind to receptors on fat cells and cause the release of cytokines. These are immune regulating molecules that travel throughout the body. The increase in cytokines will then act on the capillaries in the body-causing them to attract white blood cells. This inflammation will then restrict blood flow in these end organ vessels. This lowered tissues oxygen level also results in low VEGF. Symptoms from this can include fatigue, muscle cramps, and shortness of breath. The elevated cytokine levels can also produce flu-like symptoms of headache, muscles aches, difficultly concentrating, as well as suppression of the immune system. Lab testing at this stage may reveal elevated TNF, MMP-9, IL-1B and PAI-1.
At the same time, these cytokines including Leptin will begin to act on the hypothalamus of the brain. This is the master regulator and controller. It regulates sleep/wakes cycles, fluid levels, temperature and hunger, pain, and multiple hormones including sex hormones, thyroid hormones and adrenal hormones. The key words here are massive dysregulation. Increase leptin directly acts on fats cells causing them to store more fat and grow. At the same time, the excessive cytokines act on the hypothalamus through a feedback mechanism that works through the leptin receptors found there and destroys them. These damaged leptin receptors then fail to provide feedback that would to stimulate MSH production, and thus MSH levels fall. This is where things get messy.
Melanocyte Stimulating Hormone (MSH) is a master regulator in the hypothalamus. The downward regulatory effects of low MSH results in CIRS symptoms spiraling out of control. MSH is related to melatonin production and circadian rhythms, disrupting sleep. Endorphin production is suppressed-resulting in loss of pain control; this is commonly described by patients as Fibromyalgia type pain. Low MSH also affects the GI tracts absorption resulting in diarrhea and ‘leaky gut’. Though not Celiac Disease, some patients will develop Celiac-related antibodies (e.g. anti-gliadin IgG and IgA).
As this process continues, it starts to affect other parts of the immune system. White blood cells lose their regulation of the cytokine response-resulting in delayed recovery from illnesses. This can then lead to colonies of multiple drug-resistant Staph growing in the mucous membranes of the sinus cavities. These bacteria (aka MARCoNS) produce a toxin that further breaks down MSH and aggravates cytokine levels.
The last stage in this process is dysregulation of pituitary hormones. Low MSH can result in lower levels of ADH, a hormone that regulates thirst and urination. Patients will complain of being thirsty all the time, with excessive urination and-in the winter-describe an excessive susceptibility to static electricity shocks. Low MSH also feeds back and lowers production of sex hormones. Initially in the illness, this stress can result in elevated cortisol and ACTH but as time goes on, both levels will drop.
As you can see this is a complex process. Below are the labs and testing used to diagnose CIRS as well as determine the degree of hypothalamic dysfunction, inflammation and then to guide the treatment process. This section is more complex and laid out primarily for practitioners but again, well-educated patients should be able to get the concepts.
CIRS Evaluation Diagnostics
1. Diagnosing CIRS
Need Positive Cluster Analysis. If positive, then need 2nd (VCS) and 3rd screening positive (physical exam) OR Labs positive to get diagnosis.
2. Rule Out Other Diseases
Chronic Inflammatory Response Syndrome can be mimicked by many diseases. Before the patient and practitioner venture down this path, all other possibilities must be ruled out (through a past or present evaluation). There is extensive overlap and an experienced clinical eye is vital to ensure important diagnoses are not missed.
A partial list of rule-out diseases includes:
- Hypothyroidism
- PTSD
- Addison’s Disease
- HIV
- Chronic Infections
- Undiagnosed cancer
- Alzheimer’s Disease
- Subacute rhabdomyolysis
- Other toxin or chemical exposures
- Polymyositis
- Polymyalgia Rheumatica
- Severe nutritional deficiencies
3. Exposure
Exposure is essential for the diagnosis of CIRS but can be quite elusive at times.
Mold-Related Exposure: From history or current exposure as shown by MSqPCR (aka ERMI).
Don’t forget about the following biotoxin exposures:
- Lyme Disease
- Ciguatera
- Pfiesteria
- Reef Fish
- Brown Recluse Spider Bite
- Cyanobacteria (More to come as we continue to research this entity)
4. Labs
Need 4 positive if less than 11 years-old or 5 if greater than 11 years-old to diagnose CIRS.
- HLA DR (relative risk = susceptibility)
- MARCoNS
- MSH (regulatory neuropeptide)
- C4a (split product of compliment)
- MMP-9 (only reliable way to measure Th1)
- ADH/osmolality (loss of feedback)
- ACTH/cortisol (loss of feedback)
- TGFB
- VIP
- Antigliadin ab/Anticardiolipin ab
CIRS Panel for Pediatric patients: HLA, MSH, C4a, MMP-9, TGFB1, AGA, ACLA,
5. Visual Contrast Sensitivity Test (VCS)
This testing is highly sensitive for neurotoxins effects on the brain. 92% of those with CIRS fail the test, 8% with CIRS will still pass it, and 1% without CIRS will fail the VCS. This is a test to detect the eye’s ability to differentiate the contrast between grey and white lines of variable thickness. Those who tend to be CIRS positive but still pass are teenagers with excellent vision previously (e.g. athletes, artists, photographers).[1] This test is available online at www.VCStest.com
In the presence of CIRS, visual contrast sensitivity will decrease. We only use rows C and D for scoring a pass or fail for CIRS. These rows will show improvement as a patient is treated and biotoxins are removed. The intensification reaction from cholestyramine will show a fall in column E followed by a fall in column D. A fail in only one eye is still a fail.
For the testing to be reliable the following conditions must be met.
- Visual acuity better than 20/50
- Patient must wear their corrective eyewear
- Light must be sufficient-at least 70 foot-lamberts or more
- Patient must sit 18 inches from the screen or card
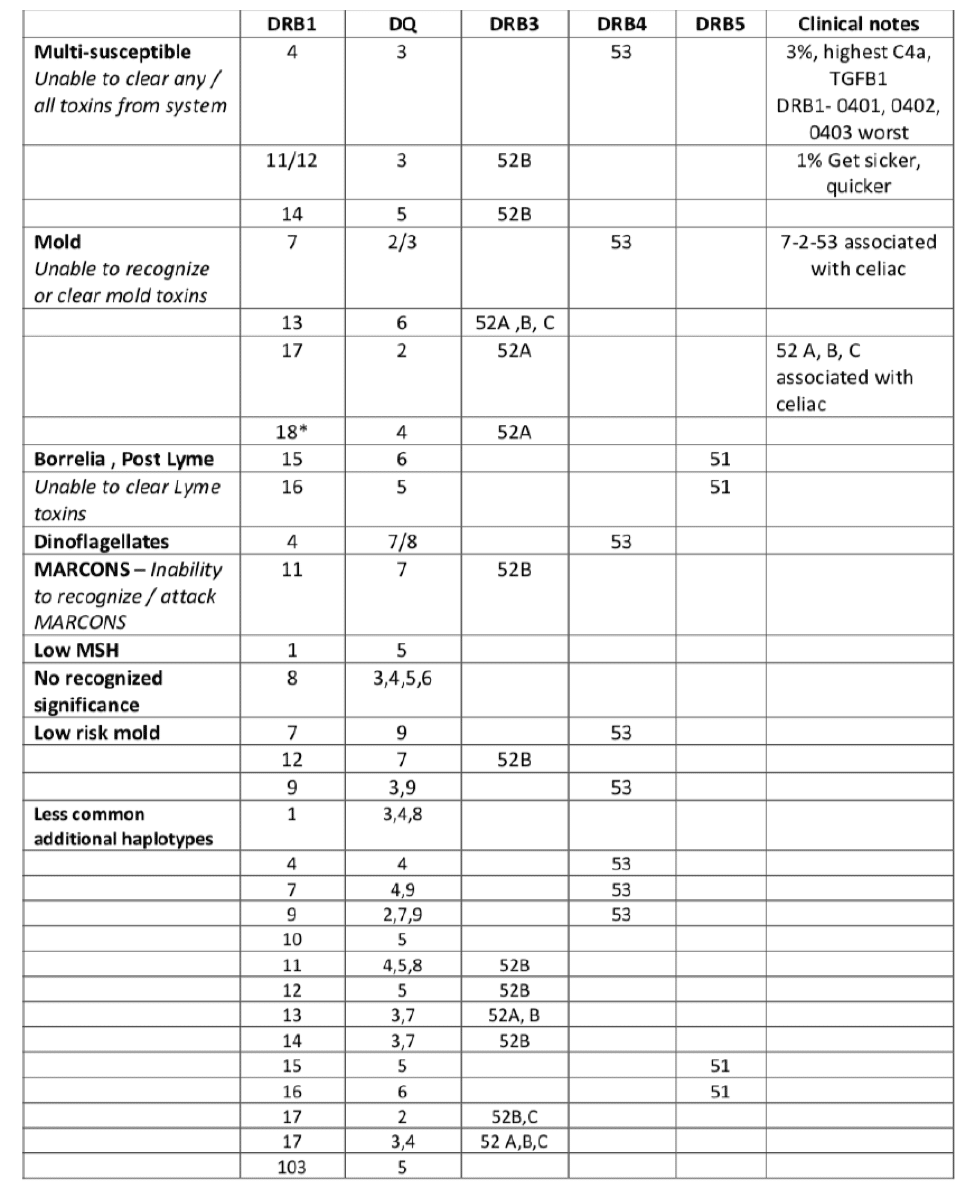
6. HLA DR/DQ Haplotype Genetic Testing
Human Leukocyte Antigens (HLAs), are located on the surface membranes of almost every cell in the body. Their purpose is to assist the immune system in identifying self versus non-self or said another way, determine what is you verses what is not you.
The immune response genes are found on chromosome six. Patients could have two alleles-copies of genes (for each gene, one allele is inherited from a person’s father, and the other is inherited from a person’s mother), out of approximately 10 possible, as part of their genotype. Based on Dr. Shoemaker’s data, in normal populations compared to international registries of gene frequencies of HLA DR, we know the frequency of mold illness-susceptible patients approximates 24% of the normally distributed population. Almost a quarter of the normal population is genetically susceptible to chronic mold illness. Three quarters isn’t.
7. Environmental Relative Mold Index (ERMI)
Mold-Related Biotoxin Exposure Testing
If there is any suspicion that a current building has water damage, an Environmental Relative Mold Index (EMRI) is crucial for determining the current health of a building. The first step in treatment requires the patient to be removed from ongoing exposure, and this test is the best way for this determination. Sampling air for mold spores has recently come under criticism due to its inability to pick up Wallemia (common mold in ducts), Stachybotrys (the dreaded black mold), and does not provide for speciation for different toxigenic molds.[3] Also, for every mold spore in the air, there are 500 particulates. So, the spore count can radically underestimate potential exposure. The IEP Consensus statement outlines in detail the weaknesses of spore trapping, so for more information refer to this resource found at the end of Part IV. Finally, ERMI does not measure all molds but those that have been shown to have the greatest importance for health implications.
Having a score of the home or building is important for several reasons. First, you want to know if the current environment is safe. Second, treatment can be foiled by recurrent exposure; if someone is not responding to treatment you need to rule out current or ongoing exposure. This is vitally important because response to therapy is the third part in the case definition of CIRS. Finally, you want to know where you started from prior to remediation. If an inspector evaluates a home and finds mold, then remediation is carried out, unless you know the starting point for the indoor air quality, all you can do is assume the initial remediation was a success. Unfortunately, at times there are still undiscovered sources of contaminates including the reservoirs found in furniture and porous materials in the home/building. Without a MSqPCR (aka ERMI) these will not be accounted for and exposure could be ongoing despite a previous remediation attempt.
The ERMI is broken into two classes: Class I represents indoor mold and Class II outdoor molds. The difference between Class II minus Class I give us the relative index between outdoor and indoor air.[4] Elevated ERMI levels have been shown to have a correlation with labs abnormalities and symptoms of those with CIRS. Below is a basic rubric for ERMI interpretation.
8. Multiple Antibiotic Resistant Staphylococcus Aureus (MARCoNS)
This organism is a slow growing bacterium that creates a sticky mucous like biofilm allowing it to stay undetected and resistant to antibiotics. It colonizes the nasal passage ways of those who have suppressed immune systems—specifically, those with a low MSH. It’s a vicious circle, MARCoNS releases endotoxin A and B which break down MSH and lower its levels and a low MSH can cause susceptibility to MARCoNS. Due to the slow growth rate of this organism, a special API Staph isolate culture is required that takes 7 days to grow. Another issue with MARCoNS is that they release a neurotoxin like that of Ciguatera which can have neurotoxic effects on the brain. Finally, inadequate treatment of this biofilm organism will reduce the efficiency of cholestyramine therapy
9. Transforming Growth Factor Beta-1 (TGFB1)
(Marker of overactive immune system)
- < 2380 pg/ml=normal
- > 5000 pg/ml = symptoms appear
- > 10,000pg/ml = restrictive lung disease, tremor, cognitive issues, joint problems may occur
- NOTE: Sample must be double spun to prevent platelet contamination
TGF Beta-1 is a protein that has important regulatory effects throughout innate immune pathways. This molecule occurs throughout the body and plays an important role in prenatal development, blood vessel formation, wound healing, formation of blood vessels, cell movement, cell self-destruction (aka apoptosis) and immune system regulation especially that affected by regulatory T-cells. Another interesting correlation is that of elevated TGFB1 and a false positive ANA. Keep this in mind when interpreting the ANA of a patient with possible CIRS.
TGF Beta-1 if not dysregulated performs a restorative function in the body. When functioning properly it helps in the regulation of muscle tissue and body fat, wound healing, immune regulation and maintenance of the blood brain barrier. When dysregulated, all these processes become affected.
Elevations of TGFB1 have been seen with a litany of fibrosing and autoimmune diseases. The following is a listing of some of those:
- Autoimmune Hepatitis
- Juvenile Rheumatoid Arthritis
- Dermatomyositis
- Pulmonary Fibrosis
- New Onset Asthma
- Scleroderma
- Pulmonary Hypertension
- Renal Fibrosis
- Systemic Lupus
- Rheumatoid Arthritis
- Ulcerative Colitis
- Learning disabilities
A final interesting piece of data about TGFB1 is that it has been associated with asthma and hypermobility. According to the EPA, 21% of all new cases of asthma may be due to exposure to water-damaged buildings. Those with Hypermobility Syndrome or EDS have been found to have a gene mutation related to fibrillin-1. This gene regulates TGFB1 and with its mutation, TGFB1 can become dysregulated and elevate.
10. Alpha Melanocyte Stimulating Hormone (MSH)
- Normal Range: 35–81 pg/mL
- If <35 there is a high likelihood of MARCoNS in those with a positive Cluster Analysis
- NOTE: The normal range reported by some labs does not separate out cases and control, so their lab range is skewed down to zero. This is incorrect.
- If MSH normal: ERMI can be >2
- If MSH <35 & C4a >20000: ERMI needs to be <-1
Melanocyte Stimulating Hormone (MSH) is a master regulator in the hypothalamus. The downward regulatory effects of low MSH results in CIRS symptoms spiraling out of control. MSH is related to melatonin production and circadian rhythms, disrupting sleep. Endorphin production is suppressed-resulting in loss of pain control; this is commonly described by patients as Fibromyalgia type pain. Low MSH also affects the GI tracts absorption resulting in diarrhea and ‘leaky gut’. Though not Celiac Disease, some patients will develop Celiac-related antibodies (e.g. anti-gliadin IgG and IgA).
Alpha melanocyte stimulating hormone is neuropeptide that controls many functions not only in the central nervous system but also throughout the body. In addition to its multiple anti-inflammatory and neuroregulatory functions it also controls peripheral cytokine release, pituitary function as well as functioning as an antimicrobial peptide affecting biofilms (like defensins).
Other functions include:
- regulating the innate immune system (potent anti-inflammatory)
- controlling pain perception through endorphins
- controlling restorative sleep through melatonin
- regulating white blood cell release of cytokines
- regulation of ACTH and ADH
- regulation of mucous membrane defenses in the sinus cavities and Gi tract
Low levels of MSH affect mainly the posterior pituitary. This results in elevated estradiol in women and low testosterone in men, as well as adrenal dysfunction.
In CIRS, MSH will be too low in over 95% of patients resulting in increased susceptibility to mold-related illness, hormone irregularities, mood swings and chronic pain.
11. C4a Levels
-
- Normal Range: 0–2830 ng/ml
- Range Interpretations:
- >20,000 is severe biotoxin illness and exquisite mVOC sensitivities
- 6000–8000 can be seen in Lyme
- Mold can be 12,000 and above
- Acute Lyme=17,000
- Chronic Lyme=8872
- Acute Mold=16,000
- Chronic Mold=12,000
- CFS=9000
- Re-exposure=19,000
C4a levels refers to part of a system known as the complement system, seen in Appendix E below. This is a group of proteins that move freely through your bloodstream and works with the immune system playing a vital role in inflammation. Each protein in the complement system actives another protein related to a select inflammatory response. This effect can spill over from the innate immune system to cause an acquired immune system response and effect multiple blood parameters. In CIRS, C4a is used to measure an excessive innate immune response to biotoxins and has become the inflammatory marker of greatest significance looking at innate immune responses in those with exposure to Water-Damaged Buildings (WDBs).
Exposure molecules know as Pathogen Associated Molecular Patterns (PAMPs) can activate the complement system. PAMP exposure can come from mold, fungi, heavy metals, infections (i.e. Lyme, bacterial or viral), and in an overtaxed system cause a ‘light switch’ phenomenon where the innate immune system become turned on but doesn’t turn off when the exposure is removed.
High or elevated C4a levels can have the following effects: cognitive deficits, restrictive lung disease, hypersensitivity pneumonitis, CFS with multi-symptom/multi-system disease, activated mast cell and basophils (sometimes referred to as Mast Cell activation), dermatographia, elevated lactate, increased smooth muscle contraction, vascular permeability, release of chemotactic factors.[5]
What do high C4A levels mean?
C4a is generated by activation of MASP2 as part of Mannose binding lectin pathway. Activated MASP2 then has the ability to auto-activate without further outside activation. Interaction with vWF polymerization leads to bleeding from mucosal surfaces (i.e. nose bleeds) and at the same time hypercoagulability. Elevated C4a levels and C3a markers for MASP2 activation can see in Lyme Disease but if no ongoing pathogen membranes are present (i.e. no ongoing infection), the C3a will not be elevated.
C4a measurement can also help differentiate a mold related exposure from a Chronic Lyme Disease state. For example, measurement of C4a before treatment can be done then repeated and 1 week after treatment with an antibiotic. If unchanged on repeat testing the patient is more likely to have CIRS, if significantly lowered this points more toward an ongoing tick related infection. C4a can also be elevated in Lupus.
C3a Levels
- Normal Range: 55–486 ng/ml
C3a is one of the more potent factors in the complement system and is present only in certain biotoxin illness patients. These include acute Lyme Disease and Systemic Lupus Erythematosus. C3a attracts and activates neutrophils which then release their contents causing vasoconstriction, increased vascular permeability and decreased tissue perfusion. Due to the actions of C3a, there is significant overlap between the complex know as Lyme Disease and CIRS from water damaged buildings.
If a patient has the HLA Haplotype 15-6-51 or 16-5-51, then they are Lyme susceptible and likely will need and extended period of antibiotics. If C3a remains elevated after antibiotic therapy and CIRS treatment, treatment with statins may be necessary to lower this inflammatory marker.
12. Matrix Metallopeptidase-9 (MMP-9)
- Normal Range: 85–332 ng/mL
This enzyme in humans is encoded by the MMP9 gene. Proteins of this family breakdown the extracellular matrix in the normal physiologic process of remodeling. This process occurs in the following: embryonic development, reproduction, and tissue remodeling, as well as in disease processes.[6] MMP-9 can be used to measure T Helper 1 cells and if low, this arm of the innate immune system is disputed. Elevation is seen in cytokine mediated inflammation where MMP-9 delivers inflammatory elements from the blood into the subintimal spaces. Elevation has been associated with diseases ranging from COPD, Rheumatoid Arthritis, Atherosclerosis, Aneurisms, Cardiomyopathy and CIRS. Elevation is also observed with increased permeability of the blood brain barrier.[7]
Matrix Metallopeptidase-9 can be used as a marker for hidden cytokine production and system intensification in CIRS when patients are given cholestyramine. Its elevation is observed in states of high toxin loads, elevated total cytokines and inflammatory disease progression. It is also increase in brain injuries, likely relating to increased blood brain barrier permeability induced by head trauma.
When drawing this lab, prechilled SST tubes should be used and it should be immediately spun down to minimize false elevations.
13. Vascular Endothelial Growth Factor (VEGF)
- Normal Range: 31–86 pg/mL
Vascular Endothelial Growth Factor (VEGF) is a sub-family of growth factors in the platelet derived growth factor family that stimulates the formation of blood vessels. This includes blood vessels formed during embryogenesis as well and ongoing angiogenesis.[8] In this fashion, VEGF restores blood circulation and oxygen to damaged tissues and helps to form collateral circulation in blocked vessels. Elevated levels signify increased activation in the innate immune system and can be seen in diabetes, renal failure, asthma, as well as tick born illness, Bartonella, cancer and asymptomatic cardiovascular disease. Its overexpression also commonly occurs in diseases of the retina.[9] Early in CIRS, VEGF levels will run high as a compensatory mechanism for oxygen delivery to hypoxic tissues but as the disease progresses, VEGF levels will fall.
In a typical biotoxin induced inflammatory response, white blood cells will accumulate with the result of reduction in distal capillary blood flow. This results in tissue hypoxia and stimulates VEGF production. It does this through Hypoxia Inducible Factor (aka HIF). Over time, compensatory mechanisms begin to fail and VEGF falls resulting in low tissue oxygen levels. Symptoms related to this tissue hypoxia include: fatigue, muscle aching, poor exercise recovery, push-crash phenomena, brain fog, air hunger and shortness of breath. Due to the change from aerobic metabolism to anaerobic metabolism, ATP production is reduced. In this state of oxygen deficient lactic acid metabolism only 2 ATP for every glucose molecule is produced, instead of 38 ATP as is norm. This affects mitochondrial ATP production and ultimately the cellular energy reserves of the entire body.
14. Vasoactive Intestinal Peptide (VIP)
- Normal Range: 23-42 pg/mL
Vasoactive Intestinal Peptide is a neuroregulatory hormone with receptors in the hypothalamus. It is made by cells found in the Suprachiasmatic Nucleus in the hypothalamus just above the Optic Chiasm. Here it receives input from the retina and olfactory bulb. This peptide regulates the peripheral cytokine response, inflammation throughout the body, pulmonary artery systolic pressure as well as having a direct effect as an endorphin. Low levels are associated with capillary hypoperfusion and shortness of breath related to elevated pulmonary artery pressures at rest and exercise
From an immune standpoint, VIP down-regulates T-helper Cell 1 responses and upregulates T-regulatory cells improving microcirculation. It has a similar role to MSH in regulating inflammation. It can also lower estrogen levels by its downregulation of aromatase and restores balance of Vitamin D (i.e. if 1,25 OH Vitamin D is high and 25 OH Vitamin D is low).
Low levels of VIP are found in 98% of patients with CIRS and only 10% on controls. A 2013 study on the use of VIP in CIRS patients found the following:[10]
- corrected estradiol and testosterone levels
- reduced refractory symptoms to control levels
- corrected the following markers: C4a, TGF beta-1, VEGF and MMP 9
- corrected T-reg cells
Prior to the use of VIP, the following criteria must be met: ERMI<2, HERTSMI-2 <10, normal VCS, negative MARCoNS.
15. ACTH/Cortisol Dysregulation
- Normal Range:
- ACTH: 8–37 pg/mL
- Cortisol (a.m.): 4.3-22.4 ug/dL
- Cortisol (p.m.): 3.1-16.7 ug/dL
- An absolute or relative dysregulation as follows may be seen:
- Absolute High: ACTH > 45 or Cortisol > 21
- Absolute Low:ACTH <5 or Cortisol <4
- Relative High: ACTH was > 15 when Cortisol was > 16 (two-tiered test)
- Relative Low: ACTH was < 10 when Cortisol was < 7 (two-tiered test)
Adrenocorticophic Hormone (ACTH) is produced in the anterior pituitary gland of the brain and controls production of cortisol, a steroid hormone, by the adrenal cortex. Cortisol naturally is increased in the morning in a circadian fashion upon awakening, utilizing glucose for brain alertness. Cortisol at 4am may be up to 1/10 that of normal at 8am. ACTH production increase in response to stressors allows for an appropriate physiological response. Excessive stress can result in sleep/wake disorders of the circadian rhythm with result of a ‘wired but tired’ feeling.
Early CIRS, as MSH levels fall, the pituitary releases high levels of ACTH resulting in elevated cortisol levels. This is a typical stress response and few symptoms are noticed. Simultaneously high cortisol and ACTH should prompt consideration in screening for brain tumor, or if simultaneously low for brain trauma (i.e. Empty Sella Syndrome). If none is found, then the dysregulation may be viewed as a symptom of neurohormonal dysregulation. This dysregulation can be found in 50% of individuals with low MSH.
16. ADH/Osmolality
- Normal Range:
- ADH: 1.3-13.3 pg/ml
- Osmolality: 280-300 mOsm
- ADH/Osmolality Dysregulations:
- Absolute High: ADH > 13 or Osmolality > 300
- Absolute Low: ADH <5 or osmolality <275
- Relative High: ADH > 4 when Osmolality 275–278 (two-tiered test)
- Relative Low: ADH < 2.2 when Osmolality 292–300 (two-tiered test)
Antidiuretic Hormone (ADH) is a peptide produced by the hypothalamus and released by the pituitary gland. The primary purpose of ADH is to maintain the concentration of the blood, as measured by osmolality, and maintain the bodies water balance. ADH also affects VIP and MSH levels in the hypothalamus, so hypothalamic regulation is tightly dependent on these three substances. Around 80% of those with CIRS will have dysregulation of the ADH/Osmolality balance. Reduced production of ADH is associated with lowered VEGF level, this lowered ADH interferes with the ability of Mast Cells to compensate for histamine driven increases in fluid volume in circulation. Low levels of ADH have been associated with Autistic behavior and the social avoidance seen in those with CIRS.
The reduced levels of ADH are related with the following symptoms of CIRS: frequent urination, increased thirst, increased static electric shocks and relative dehydration with migraine headaches. Correction of ADH with DDAVP can initially lead to edema with rapid weight gain from the fluid retention.
17. Anti-Gliadin IgA/IgG
- Normal Range: 0-19 ACLA IgA/IgG/Ig
- MNormal Range: IgA <12; IgG <10; IgM <9
Antigliadin (AGA) antibodies are a marker for increased gastrointestinal permeability (i.e. Leaky Gut) and increased risk for autoimmunity. When MSH is low, there is increased intestinal permeability which can lead to a loss of the gut integrity and increased autoimmunity. When this occurs, multiple autoantibodies can be observed which include AGA and ACLA. A full Celiac panel can be used to rule out Celiac Disease (i.e. anti-Endomysial antibodies with anti-Tissue Transglutaminase antibodies) verses just the gluten sensitivity with positive AGA. Antigliadin antibodies are found in over 58% of children with CIRS.
Anticardiolipins (ACLA) are another autoantibody associated with CIRS. These are antibodies that become directed against one’s own body. These specifically disrupt the normal function of blood vessels and proteins bound to phospholipids in the vessel walls. The IgA, IgM and IgG of ACLA can be associated with collagen vascular diseases such as Lupus and Scleroderma as well as Auto-phospholipid Antibody Syndrome. These specific autoantibodies are found is over 33% of children with CIRS.
Other Useful Labs/Tests
Leptin
- Normal Range (Male): 0.5–13.8 ng/mL
- Normal Range (Female): 1.1–27.5 ng/mL
Though an important player in Biotoxin Related illness, Leptin is not one of the official diagnostic markers. From the Biotoxin Pathway, leptin activates MSH production in the hypothalamus. Receptors for leptin can be damaged by toxin induced cytokines. High levels of leptin result in the increased storage of fat in adipose cells, resulting is uncontrolled weight gain that tends not to respond to typical diet changes. Elevated leptin can increase the production of TNF alpha, IL-1, IL-6 which are all typically downregulated by MSH.
Other Autoantibodies
ANA, MBP, F Actin, ANCA, Anti-Phospholipid antibodies
These are other autoantibodies that have been associated with CIRS but are not considered as primary diagnostic criteria.
NeuroQuan 3T MRI
This is a newer technology that was approved by the FDA in 2006. This utilizes new 3T MRI technology with a special protocol of more frequent thinner slices. This then enables a computer software program to calculate the volume of the regions of the brain and compare then to that of an age matched normalized population. This allows for minute changes in the brain, that are imperceivable to a radiologist, to be picked up. Then using the volumetric data, changes associated with CIRS-Water Damaged Building, CIRS-Lyme pattern or TBI can be elucidated. The technology also is being used to help determine potential causes in those with Alzheimer’s Disease.
Testosterone/Estrogen/Androgens
Low MSH can result in the upregulation of aromatase. This can increase estradiol and other estrogen levels and lower testosterone and DHEA.
vonWillibrand Profile
Acquired von Willebrand syndrome can result from elevated levels of C4a and cause both bleeding tendencies (i.e. blood nose) as well clotting abnormalities (i.e. DVT and pulmonary emboli).
PAI-1
Marker for increased blood coagulation.
Genomics
Genomic analysis allows the measurement of the actual activation and activity of the human genome through the measurement of mRNA and iRNA. These transcriptomic patterns can then elucidate metabolic patterns of cellular function. There are several key immune regulators that are known to be differentially activated in those with CIRS: CD244, CD3D, CD48, CD52, granzymes, defensins and the Ikaros family. As the field of human genomics advances, the actual measurement off pre and post-treatment gene expression will be revolutionary.
Stress Echocardiogram
Part of the evaluation for CIRS is to rule out other disease processes. This includes cardiovascular as well as pulmonary diseases. A cardiac echo can elucidate the resting pulmonary arterial pressure and then compare that to the post-exercise pressure. A rise of >8 in the PASP is a marker for increased pulmonary artery pressures which is seen in CIRS.
References
- Shoemaker R, Hudnell K. Possible Estuary-Associated Syndrome: Symptoms, Vision and Treatment Environmental Health Perspectives Vol 109. No5 May 2001.
- Shoemaker R. Surviving Mold. Otter Bay Books 2010. pp744-746.
- Lin K-T, Shoemaker R.C. Inside Air Quality Filtration News Vol 26, No 3, pg. 32, 2007
- Ibid
- Ogata RT, Rosa PA, Zepf NE. Sequence of the gene for murine complement component C4a. The Journal of Biological Chemistry, 1989; 264(28): 16565-72
- Shoemaker RC. Defining Sick Building Syndrome in adults and children in a case-control series as a biotoxin-associated illness: American Journal of Tropical Hygiene and Health; 2005;73 (6):228
- Candelario-Jalil E, Thompson J, Taheri S, Grossetete M, et al. Matrix metalloproteinases are associated with increased blood-brain barrier opening in vascular cognitive impairment. Stroke. 2011 Mar 31
- Palmer, Biff F.; Clegg, Deborah J. (2014). “Oxygen sensing and metabolic homeostasis”. Molecular and Cellular Endocrinology. 397: 51-57. doi: 10.1016/j.mce.2014.08.001
- Cooper, Mark; Dimitria Vranes; Sherif Youssef; Steven A. Stacker; Alison J. Cox; Bishop Rizkalla; David J. Casley; Leon A. Bach; Darren J. Kelly; Richard E. Gilbert (November 1999). “Increased Renal Expression of Vascular Endothelial Growth Factor (VEGF) and Its Receptor VEGFR-2 in Experimental Diabetes” (PDF). Diabetes. 48 (11): 2229-2239. doi:10.2337/diabetes.48.11.2229. Retrieved 6 November 2013
- Shoemaker RC, House D, Ryan J. Vasoactive intestinal polypeptide (VIP) corrects chronic inflammatory response syndrome (CIRS) acquired following exposure to water-damaged buildings. Health, 2013; 5 (3) 396-401
Free Resource from Harvard School of Public Health
"*" indicates required fields


Take Back The Outdoors
Get the relief you need:
- Blocks 96% of histamine release BEFORE symptoms start
- Works within 14 days (critical for beating peak pollen season)
- Includes the exact formulation that delivered results in clinical studies
- Has helped 12,549 allergy sufferers enjoy spring without medications
Don’t wait until you’re already sneezing. The prevention window is closing.
10% discount through Fullscript. First-time buyers save an additional 15%.
WAIT: Skip the Reading & Get the 96% Allergy Solution Now
No time to read? I get it: You don’t need another article—you need relief.
Let me take you directly to my protocol that:
- Blocks 96% of histamine release BEFORE symptoms start
- Works within 14 days (critical for beating peak pollen season)
- Includes the exact formulation that delivered results in clinical studies
- Has helped 12,549 allergy sufferers enjoy spring without medications
Don’t wait until you’re already sneezing—the prevention window is closing.
10% discount through Fullscript. First-time buyers save an additional 15%.