CIRS: A New Paradigm for Chronic Disease | Part 2
Diagnosing CIRS

Aaron Hartman MD
November 13, 2018

Subscribe
Never miss out on new content from Dr. Hartman.
Steve had already seen five different specialists. How was I going to diagnose him appropriately and not simply label him with another medical malady? What set of scientifically proven criteria could I use to accurately diagnose him with at least 99% certainty, that other practitioners have already been using, and to date has diagnosed over 10,000 patients?
What we are going to review next are the systematic criteria used to diagnose CIRS and taking a look at CIRS symptom clusters. In Part 3, I will discuss in detail both the Biotoxin Pathway and the related labs used to diagnose CIRS. These two articles are intended for those who want to know more about the basic science behind this disease.
CIRS Diagnosis — Tier One:
History of Exposures
The first diagnostic tier begins with a history of exposure. This could be to any one of the following biotoxins:
- Water Damaged Building (WDB)
- Pfiesteria
- Ciguatera
- Red Tide
- Blue Green Algae
- Black widow or brown recluse spider bite
- Tick bite or tick born illness.
History of exposure can be a bit tricky, however. The exposure may have been years prior, as in Steve’s case. Or, it could be ongoing in the patient’s current home, school, or workplace. The difficulty with a history of exposure is that many sources of mold are hidden and the types of biotoxins unknown. Sources of mold can be from a water leak under a sink or at a hose bib; condensation in a HVAC unit or from ductwork in the home; or just from a high relative humidity in the home. Other biotoxins could include an unseen tick bite from the recent past or a huge chlorine exposure at a recent pool therapy session (as in one of my other patients).
After establishing whether or not there has been a past exposure to a WDB (which is the case in 80% of CIRS patients), the next step is to test the current home for water damage. This is best done with a MSqPCR (Mold Specific Quantitative PCR) commonly referred to as an ERMI (Environmental Relative Mold Index). When unsure if there is an ongoing exposure, testing for particulates with a mold specific quantitative PCR (aka ERMI) is needed. The details for this will be discussed in the testing section.
Symptom Cluster Analysis
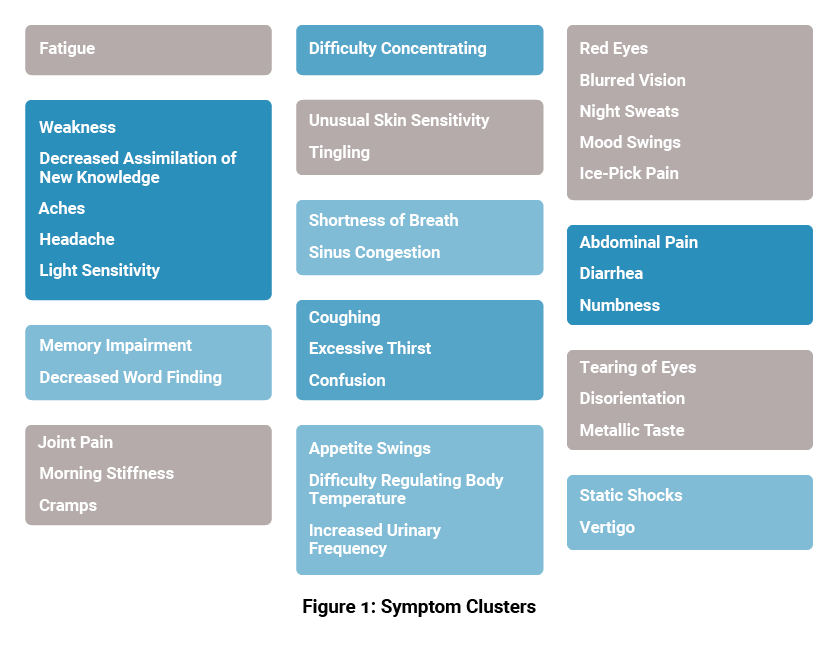
Once exposure has been verified, symptoms must be elucidated in a systemic rubric called a Cluster Analysis. It is based on symptom clusters (Figure 1). By definition, a patient needs to meet a multisystem, multisymptom screening analysis and it must be performed by an experienced clinician. This is due to the nuanced complexities of CIRS. When performed correctly, the Cluster Analysis has an accuracy of 95% in identifying patients at risk for CIRS.
A finding of any symptom in a category earns the patient one point. There are thirteen categories. Six or more points are considered diagnostic for children and eight or more diagnostic for teens and adults. The Cluster Analysis symptoms and categories are as follows:
CIRS Symptom Cluster Analysis Categories
- Fatigue
- Weakness • Assimilation • Aching • Headache • Light Sensitivity
- Memory • Word Finding
- Concentration
- Joint Pain • Morning Stiffness • Cramps • Clawing
- Unusual Skin Sensations • Tingling
- Shortness of Breath • Sinus Congestion
- Cough • Thirst • Confusion
- Appetite Swings • Body Temperature Regulation • Urinary Frequency
- Red Eyes • Blurred Vision • Sweats • Mood Swings • Ice Pick Pains
- Abdominal Pain • Diarrhea • Numbness
- Tearing • Disorientation • Metallic Taste
- Static Shocks • Vertigo
So, for example, a person complaining of fatigue (#1), brain fog, problems concentrating (#4), joint pain, stiffness, cramping (#5), weird skin sensations, tingling (#6), shortness of breath (#7), mood swings, blurred vision (#10) and vertigo (#13) would have 13 symptoms in 9 categories and have a positive Cluster Analysis screening.
If a patient gets enough points to be considered diagnostic, the screening continues to the VCS test.
CIRS Diagnosis — Tier Two:
CIRS Testing, Exam, & Labs
Second tier screening begins with a CIRS test called the Visual Contrast Sensitivity Test or VCS for short. If a patient meets the Cluster Analysis AND fails their VCS, the diagnostic accuracy of these two tests reaches 98.5%. Though not required, a positive VCS is helpful to determine the diagnosis, if treatment is working and if a patient gets re-exposed throughout the course of their illness.[1]
Next, the second tier process involves a physical exam and lab testing group. There are several subtle findings on the physical exam. Typically, the exam is considered ‘normal’ by the lack of specific hard findings. The utility of the physical is largely to rule out other disease entities. The following ‘soft signs’ that are not diagnostic but frequently encountered include the following:
- Red eyes
- Hyper-flexibility,
- Wingspan exceeding height,
- Resting tremor
- Cool Hands and Feet
- Pallor
- Discolored Hands and Feet
- Decreased muscle strength in hands and feet
- Decreased muscle strength in shoulder flexion
- Decreased tidal volume
- Dermatographia
- Nasal polyps
- Asymmetric peripheral neuropathy
- Cranial nerve palsies (III, IV, VI, VII)
After the initial evaluation, a full lab panel is ordered to rule out other disease entities as well as evaluate a patient for CIRS. That full panel is available here. In tier two, a patient must have 4 or more abnormal labs if they are <11 years old and 5 or more if they are 11 years old or more and a normal exam or one with the subtle findings above.
The following tests are the core labs in the tier two CIRS testing:
- HLA DR/DQ gene testing
- VIP, MSH, ADH/osmolality, ACTH/cortisol
- TGFB1
- MMP-9
- MARCoNS
- ACLA/AGA
- C4a
Once these criteria are met, the patient moves onto Tier Three.
CIRS Diagnosis — Tier Three:
Diagnostic & Therapeutic Trial
Tier Three is considered a diagnostic and therapeutic trial. A patient with CIRS, meeting Tiers I and II should respond to treatment. Their symptoms score should diminish with time, their VCS should normalize, and their labs should improve. If a patient is not responding, either the wrong diagnosis has been made or there is ongoing exposure to WDB or another source of biotoxins. The clinician’s role here is to help the patient understand where there may be an unknown exposure and address it. At this point, if not already done, home and work place MSqPRC should be performed to rule out current exposure. If there is none, a repeat evaluation and examination should be performed to determine if another diagnosis is appropriate in the patient’s case.
The above is the basic rubric used for diagnosis of CIRS. This is a complicated process for both clinicians and patients. Resources available for patients include the recently published MOLD ILLNESS: SURVIVING AND THRIVING, A Recovery Manual for Patients & Families Impacted By CIRS by Paula Vetter , Cindy Edwards and Laurie Rossi For practitioners there are two consensus statements, one for the medical side of treatment and care and the other for evaluation of the home and remediation. These resources are required reading for both practitioners as well as patients.
In Part 3, I will take a deep dive into the Biotoxin Pathway to describe the disease process of CIRS more fully as well as into the labs, their interpretation and meaning. This section will be complex but is encouraged reading for anyone wishing to know more about this common and potentially devastating disorder. Following the entire evaluation and treatment protocol that follows will require a re-orientation of an individual’s thoughts, actions and lifestyle. Few will start the process and fewer still will complete it. But for individuals with CIRS this may be the only way to regain health. What I have put together in this four-part series is intended as a primer. It in no way replaces working with a skilled experienced clinician who has worked with difficult cases in the past. At the end of Part IV will be additional resources that can help both the patient and professionals that are working with them. Please make use of these. The more education the better. The more you understand what is going on in your body and what others have gone through, the better equipped you will be to make this journey. This kind of medicine requires the patient and family to be active participants in their care. The clinician will guide them through this arduous process. At the same time, there are many resources out there that are subpar and only superficial in their approach and understanding of CIRS. After reading Parts III and IV, please review all the resources that follow. These will enable you to become engaged in your health care an empowered in the struggle it will be to work through this process.
References
- Shoemaker, Johnson, et all. Diagnostic Process for Chronic Inflammatory Response Syndrome (CIRS): A Consensus Statement Report of the Consensus Committee of Surviving Mold. Internal Medicine Review 2018: p27.
Free Resource from Harvard School of Public Health
"*" indicates required fields


Take Back The Outdoors
Get the relief you need:
- Blocks 96% of histamine release BEFORE symptoms start
- Works within 14 days (critical for beating peak pollen season)
- Includes the exact formulation that delivered results in clinical studies
- Has helped 12,549 allergy sufferers enjoy spring without medications
Don’t wait until you’re already sneezing. The prevention window is closing.
10% discount through Fullscript. First-time buyers save an additional 15%.
WAIT: Skip the Reading & Get the 96% Allergy Solution Now
No time to read? I get it: You don’t need another article—you need relief.
Let me take you directly to my protocol that:
- Blocks 96% of histamine release BEFORE symptoms start
- Works within 14 days (critical for beating peak pollen season)
- Includes the exact formulation that delivered results in clinical studies
- Has helped 12,549 allergy sufferers enjoy spring without medications
Don’t wait until you’re already sneezing—the prevention window is closing.
10% discount through Fullscript. First-time buyers save an additional 15%.