Superpower or Supersyndrome? | Part 2
Hypermobility & Chronic Health Issues
Connecting the Dots between Chronic Fatigue, Autoimmune Disease, & POTS

Aaron Hartman MD
April 9, 2024

In my previous article on hypermobility, I noted my surprising discovery of a single predisposing factor associated with the most common & complex issues doctors address every day. Time and time again, I observed that hypermobility is the common denominator in a host of medical issues patients grapple with: chronic fatigue, fibromyalgia, dysautonomia and POTS, autoimmune diseases, gut issues, chronic Lyme, mold toxicity, even long COVID.
How can this be?
Is Hypermobility a Supersyndrome?
Syndrome: a group of symptoms which consistently occur together, or a condition characterized by a set of associated symptoms.
If a syndrome is a condition associated with a cluster of symptoms, a supersyndrome is a group of related conditions often seen together. Is hypermobility just such a supersyndrome? You can probably guess the answer already.
Hypermobility affects the whole body. If your joints are hypermobile, all the connective tissue in your body is also hypermobile. This includes your gut, neck, and immune system, just to name a few. That is why hypermobility can be the root cause of many issues. I see these four conditions in many of my patients that are hypermobile.
I will not attempt to cover every condition that may be related to or caused by hypermobility. Instead, I would like to look at three specific conditions:
- Chronic Fatigue
- Autoimmune Disease
- Dysautonomia & POTS
I trust you’ll see a lot of overlap and connections between these and many other “mystery illnesses” … maybe even some of the issues you’re struggling with. If you’re like many people I have worked with, you know that there is something behind all these weird issues. But you haven’t yet been given the framework to connect the dots.
That framework may just be hypermobility. Let’s look at three seemingly unrelated medical conditions.

Chronic Fatigue
What is the difference between fatigue and just being tired?
Many people deal with fatigue, which is much different from simply being tired. Tiredness is usually related to exertion from exercise or not having a good night’s sleep. After a day or two of rest, we usually recover from tiredness. Fatigue lingers.
I often see patients who have both chronic fatigue and hypermobility. If you’re hypermobile and have experienced chronic fatigue, know that you’re not alone. It’s not a coincidence, and it’s not just all in your head. There is indeed a link between fatigue and hypermobility.
Let’s look at ten reasons why hypermobility can increase your risk for fatigue (and what you can do about it).
10 Reasons Hypermobility Leads to Chronic Fatigue
-
Ligament Laxity
- The Problem: If you’re hypermobile, then your joints are a bit loose. When you sit in a chair, then, you cannot rely on your ligaments and tendons to hold your body in position. You have to contract your muscles to compensate. Your muscles, therefore, need to chronically contract simply to keep your joints in place. This excessive load places an increased energy demand on your system.
- Solutions: Muscle-strengthening exercises like pilates can provide the core strength required for seemingly simple tasks. Be sure to take regular breaks throughout the day
-
Autoimmune Dysfunction
- The Problem: Autoimmune issues are a common characteristic of hypermobility (to the extent that we use autoimmune issues as a diagnostic for hypermobility). Basic lab testing for auto antibodies are used to diagnose these. The underlying inflammation related to the immune system commonly causes fatigue, as well as mitochondrial dysfunction (energy production at the cellular level).
For more information on this topic, check out these blog posts on autoimmune issues
- The Problem: Autoimmune issues are a common characteristic of hypermobility (to the extent that we use autoimmune issues as a diagnostic for hypermobility). Basic lab testing for auto antibodies are used to diagnose these. The underlying inflammation related to the immune system commonly causes fatigue, as well as mitochondrial dysfunction (energy production at the cellular level).
-
Nutrient Deficiencies
- The Problem: Most of the population is already deficient in key nutrients, but people with hypermobility have a greater need for specific nutrients such as collagen, trace minerals, and vitamin C. Blood testing will often come back “normal” because the deficiency is considered mild, but fails to account for higher levels required by people with hypermobility.
- Solutions: Supplement with B vitamins, folic acid, carnitine, creatine, or niacin to supporting the mitochondria in energy production.
-
Anemia
Anemia is somewhat of a sub-category of the nutrient deficiencies noted above.
- The Problem: Anemia is a bit unique for people with hypermobility. I often see “normal” hemoglobin levels (12-15), but with low ferritin (less than 60). Although the hemoglobin is normal, they have low active iron in their body. Iron is important for liver function, brain function, detoxification, and transporting oxygen to the cells. Many patients have low-grade fatigue that can simply be addressed by iron supplementation.
- Solutions: I tend to recommend liver powders or extracts for this because they do not cause constipation and GI distress, as many iron supplements do.
-
Sleep Apnea
I frequently see sleep apnea in my hypermobile patients.
- The Problem: People with hypermobility have laxity of the soft tissue throughout the body, including in their throat and/or trachea, which can cause them to collapse easily during sleep. People with hypermobility also tend to have narrower airways which can cause mild sleep apnea. I call this “skinny people sleep apnea” because most of these patients are not overweight. They look healthy. They don’t look like normal candidates for sleep apnea, but they have it nonetheless.
- Solutions: If you have hypermobility, consider a sleep study to check for sleep apnea.
-
Inadequate Restorative Sleep
While sleep apnea can cause sleep deprivation, there are other reasons that a hypermobile person might not be getting the quality sleep that they need.
- The Problem: Increased stressors in the body lead to chronically elevated cortisol. The body can’t get out of fight-or-flight mode and into a rested state to sleep and repair.
- Solutions: Magnesium supplementation, meditation, and prayer before going to bed can be very helpful here. Managing light exposure is also important for restful sleep. Getting at least 10 minutes of natural light in the eyes in the morning and avoiding blue light two hours before going to sleep can help reset the circadian rhythms for better sleep patterns. Phosphatidylserine, Relora, ashwagandha, and magnesium salt baths, just to name a few, are some things that can lower your sympathetic tone, so you can get a good night’s rest.
-
High or Low Intracranial Pressure
- The Problem: Intracranial pressure is simply the pressure inside the head. This is common in people with hypermobility due to instability in the joint between their skull and spine. This is referred to as atlantoaxial instability. Cervical instability, which is excessive movement in the first and second vertebrae of the neck, can also cause issues with pressure inside the head. The ducts in that part of your brain that allow cerebral spinal fluid to flow are compressed and the pressures can become relatively elevated. Also with hypermobility, sometimes small micro tears form in the lining of your lower spine, resulting in small leaks and low back pain — commonly seen after epidurals — which can result in low intracranial pressure. Both of these affect the function of the brain, blood flow to the brain, and hormonal function which can all result in low-grade fatigue.
-
Hormonal Dysfunction
- The Problem: Hormonal dysregulation is very common in hypermobility. This can be for many reasons including underlying inflammation, nutrient deficiencies, and increased intracranial pressure. These can all affect your pituitary which is the center of hormone regulation. Many people refer to this as the HPGA (hypothalamus pituitary gonadal) axis.
-
Mast Cell Activation Syndrome (MCAS)
While you may not have heard of MCAS, 20 – 30% of the population deal with some degree of it, according to Dr. Afrin, the leading scientific researcher on MCAS. We’re just now learning of this syndrome, which can include things like hives of unknown reason, tongue swelling, angioedema, and uncontrolled itchy skin. Sometimes anxiety flares, panic attacks, and a racing heart can result from MCAS.
Mast cells are cells that release histamine in your body. Typically the innate immune system attacks and destroys viruses, particulates, toxins, etc, and then activates mast cells which release inflammatory mediators. What is interesting about mast cells is that when they leave the bone marrow, they have not yet taken their final form. If they go to your bladder, for example, they can cause interstitial cystitis. In your brain, however, mast cells can cause inflammation leading to chronic fatigue and fibromyalgia. You get stuck in this inflammatory, feed-forward process. New research suggests that hypermobility might be primarily caused by early mast cell activation syndrome.
-
Orthostatic Intolerance (POTS)
- The Problem: POTS is another disorder that commonly overlaps with hypermobility. I’ve included a full section on Dysautonomia, POTS, & hypermobility below. Lower blood flow to the brain and body cause low-grade fatigue; exertion makes the fatigue worse.
- Solutions: The basic four tenets to treat POTS are adequate fluids, electrolytes, compression, and exercises to help build muscle (See the section below).
Autoimmune Disease
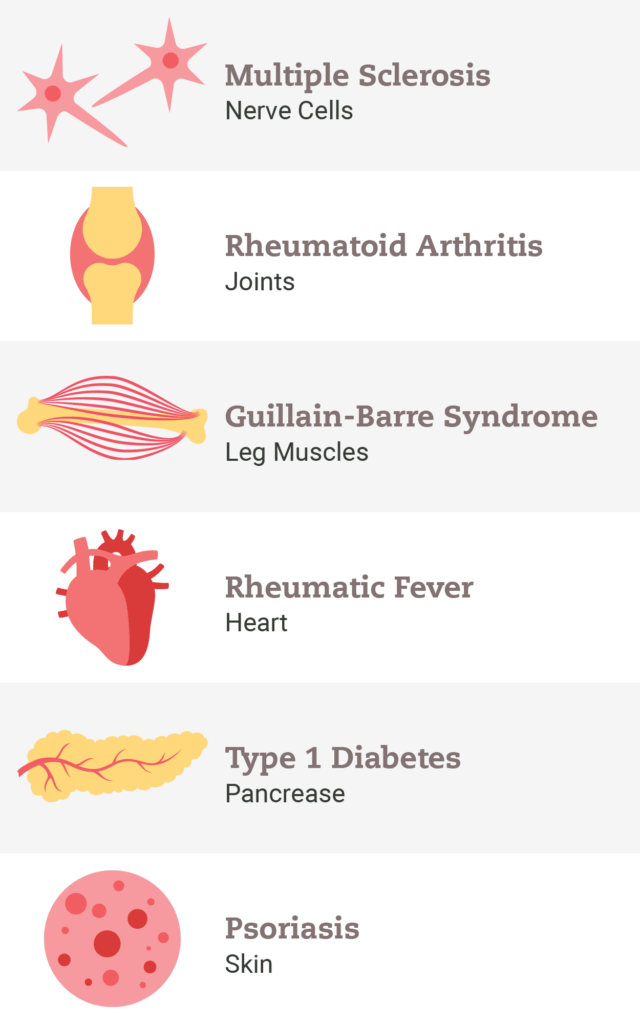
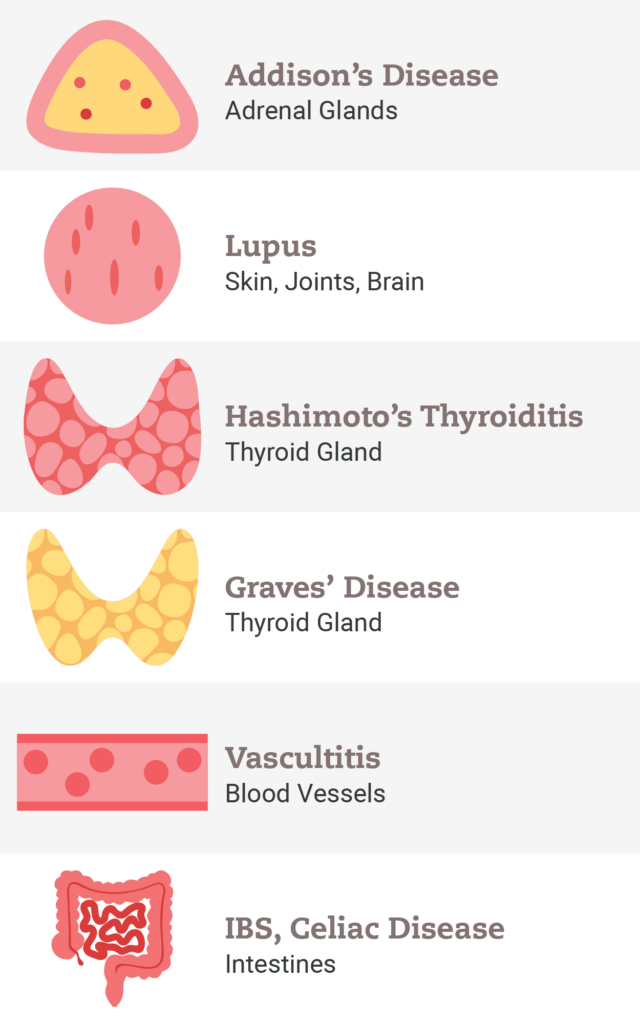
One in 12 Americans have an autoimmune disease of some sort, and another 20% of Americans have a positive autoantibody. You probably know someone who has an autoimmune disease. When I see a patient with Hashimoto’s, Rheumatoid Arthritis, Crohn’s disease, Colitis, or any autoimmune disease, I always consider whether they have any associated syndromes, and whether they are hypermobile.
Autoimmunity is a dysregulation of the immune system. The immune system can become overreactive. If the immune system becomes oversensitive to pollen, dust mites, toxins, or other environmental triggers, we get allergies and/or asthma. If the immune system becomes overreactive to bacteria or yeast on the skin, we might experience eczema. In the same way, rosacea and acne can be caused by SIBO (small intestine bacterial overgrowth). We’re just now understanding that this includes things like PCOS (polycystic ovarian syndrome), IBS (irritable bowel syndrome), and IBD (inflammatory bowel disease). These are all part of the autoimmune spectrum.
But what are the chain of conditions that lead from hypermobility to autoimmune disease?

Hypermobility Contributes to Leaky Gut
About 30% of Americans complain of some kind of gastrointestinal issue, which is the most common reason that people see a GI doctor. If I see someone with gut issues, bloating, gas, or if they often have food that gets stuck in their throat, have very slow digestion, or constipation, I always consider whether hypermobility might be at the root of these issues. But what is the connection between hypermobility and the gut?
Did you know that many people with hypermobility also have something called visceroptosis? This is a medical term that describes the sinking or prolapse of the abdominal organs. Because of loose joints and ligaments, the abdominal organs aren’t held in place as securely. The pressure of these organs affects gut motility and also increases bacterial and yeast overgrowth. So this visceroptosis by itself can induce leaky gut syndrome and increase gastrointestinal permeability, which is a major contributor to autoimmune disease.
So hypermobility results in “saggy bowels,” which results in leaky gut, which in turn results in autoimmune disease.
Hypermobility Leads to Elevated Cortisol
Did you know that people with hypermobility have a larger amygdala? Since the amygdala regulates emotions, people who are hypermobile often also have an increased level of alertness or arousal. These people tend to have stronger emotional memories, and their bodies can overreact to stimuli. This can be a helpful trait, as being hyper-alert to your environment could be beneficial in a survival situation. However, in today’s culture, it often results in elevated cortisol. Chronically elevated cortisol can result in more leaky gut and also tends to drive the immune system to be more reactive and to increase the antibody response.
Can you guess which hormone is the only hormone in your body that increases with age? That’s right – it’s cortisol. Other hormones like thyroid, sex hormones, and insulin tend to decrease with age, but cortisol tends to go up. So you can see how this could be particularly problematic for hypermobile people who already have elevated cortisol.
Solutions & Strategies
We know that 20% of Americans have a positive auto antibody. I had a positive AMA for about four years. With a lot of personal work, cleaning up my environment, and healing my gut, I was able to clear it. You can do this too! Stress management, gut health, diet, and environmental factors all become super important in addressing and preventing autoimmune issues.
This emerging research is illuminating the connections between hypermobility, gut issues, and autoimmune disease.
Dysautonomia & POTS
Dysautonomia is a dysregulation between the sympathetic nervous system (fight or flight) and the parasympathetic nervous system (rest and digest). It’s a sympathetic overdrive and a parasympathetic underdrive.
Symptoms of Dysautonomia Include:
- Dizziness
- Lightheadedness
- Fast heart rate
- Low blood pressure
- Edema
- Slow gut transit
To understand the four phases of dysautonomia, we need to have a basic understanding of the vagus nerve. So, let’s begin there.
What is the Vagus Nerve?
The vagus nerve runs from the brain to the organs, the GI tract, and various other areas of the body. It helps control the heart rate and regulates digestion. The body uses the vagus nerve to transmit information both ways, so this nerve also tells the brain what is going on in the organs. Your vagus nerve is the main rest and digest, calming nerve. When we take deep breaths through the belly, we are activating the vagus nerve. In medical school, I learned that, when people have a fast heart rate, giving a carotid massage can slow it down, because the massage activates the vagus nerve.
Now that we understand the basic function of the vagus nerve, let’s talk about the four phases of dysautonomia, which is a vagal tone dysfunction.
Four Phases of Dysautonomia
Phase I
The first phase of dysautonomia is just a pure vagal tone dysfunction. This generally starts in the brain, sometimes with a concussion, head injury, or a traumatic event. In this case, blood pressure might be slightly low with a slightly higher pulse rate. The person might be experiencing mild anxiety. Some people remain in this phase one to four months and even never progress. Others do progress if additional stressors add burden to the body, such as living in a moldy building, gut issues, or nutrient deficiencies. Even triggers like tick bites can escalate dysautonomia from phase one to phase two.
Phase II
Phase two is relative hypovolemia, which just means low volume. As blood begins to pool in the feet, the person can experience mild edema, and their feet might look a little mottled. The kidneys respond to an increase in fluid, while the brain tries to get more blood flow. So the person would experience a higher heart rate, low blood pressure, and frequent urination.
It’s almost like half of the body is not communicating with the other half. I’ll hear these patients say they drink lots of water, but it goes right through them. That’s when I pause to consider whether they could have dysautonomia, perhaps related to hypermobility.
When this low volume status is exacerbated, lower blood flow to the brain, gut, heart, and other organs results. Brain fog and poor sleep then follow. If there is an underlying pain syndrome, it can get worse, because of decreased blood flow to the muscles. Muscles fatigue more easily and can become somewhat achy in this phase.
Phase III
The next phase is metabolic dysfunction. It’s logical that the metabolism would slow down as a result of low blood flow. Blood pressure and blood sugar become more difficult to regulate. Mast cell activation syndrome (MCAS), metabolic syndrome, or even mitochondrial dysfunction can result. These patients are much more sick and experience a host of systemic symptoms.
Phase IV
This phase can begin 12 – 24 months after the first phase of dysautonomia. In phase four, early symptoms of hypermobility spectrum disorder become more problematic. Loose joints become even more loose because connective tissue is not being repaired quite as well. The autonomic nervous system continues to malfunction and may be so suppressed that these patients have difficulty recovering from minor illness or anesthesia.
These are the four stages of dysautonomia that I look for. They help me to gauge the seriousness of a patient’s illness and how aggressive I should be with interventions. There are many strategies I use when treating dysautonomia. I often use IV fluids, nutritional interventions, mind-body therapy, stress reduction, trauma therapy, gut protocols, sleep-wake cycles, and pain treatment if necessary.

What about POTS?
Postural Orthostatic Tachycardia Syndrome (POTS) is a type of dysautonomia, which I see frequently in my clinic and which commonly coincides with hypermobility. The “P” in P.O.T.S. stands for “Postural” which just means a change in posture. In other words, POTS is dysautonomia when your posture changes.
There is a simple test you can do yourself to see if you might have POTS. It’s called the NASA Lean Test, and you can Google it and do it at home! Basically, you check your blood pressure and pulse after lying down for a few minutes. Then you sit up and check it again a couple of times. Then you stand against a wall and recheck it. If there is a significant change in blood pressure and/or pulse as your positioning changes, you may have POTS. There are other ways to assess for POTS as well, but this is a simple test that anyone can do at home.
Solutions: The basic four tenets to treat POTS are adequate fluids, electrolytes, compression, and exercises to help build muscle.
Conclusion
It took me a while to connect the dots between hypermobility and so many other conditions. By and large, the medical community still isn’t paying attention to hypermobility. It’s starting to work its way into the medical literature. Medicine will catch up, eventually. But I don’t want you to go through many years of discovery … especially if you’re facing several conditions. I don’t want you to be largely ignored by all the specialists.
The first step, of course, is to figure out whether you are, in fact, hypermobile. We’ve put together a simple quiz to help you answer that question.
Are You Hypermobile?
Take the ConnectCODE Self Assessment to discover your individual ConnectCODE, and what impact hypermobility may have on your health.